Shoulder Injury Prevention for Baseball Players
The Problem

The Holy Grail for MLB teams is the 100 mph pitch. Once a luxury, now a necessity. In fact, probably each MLB team has one flame-hurler who can dazzle the crowd with such a performance. Spectators used to be awed by home runs, now their eyes are glued on the stadium radar gun reading of a 100-mph pitch as the slam dunk of baseball everyone wants to see.
No less impressive are those laser projectile throws by positional players, sometimes in midair under compromised body positions. Baseball is a game where 90% of the time, if the ball is in the glove, the player’s job is to throw it somewhere else as fast as possible.
However, the price paid is that 40-60% of all competitive baseball players have suffered shoulder pain at one time or another, and one in five of those injured athletes continue to play in spite of shoulder pain. It is not uncommon for many athletes to have had shoulder surgery, even multiple times.
Overhead athletes, such as volleyball players, tennis players, and swimmers are all at risk for shoulder injury; baseball players are particularly prone. Diagnoses such as “impingement”, “bursitis”, “tendinitis”, “labral tear”, “SLAP tear”, “hyperlaxity”, “instability”, and “rotator cuff tear” have become household terms. The repetitive overhead arm motion in pitching and throwing cause tremendous amount of stress to the rotator cuff muscles and tendons.
Functional Shoulder Anatomy
The shoulder, being the most mobile joint in the body, endows our ability to place our hands virtually anywhere in space. In exchange for this evolutionary trait of nearly unrestricted arm motion, by default, comes with increased shoulder instability. Unlike the very stable hip joint, the shoulder joint is not secured by a bony socket. This has been compared to as a golf ball (the humeral head) sitting on top of a “tee” (the glenoid). But, realistically, whenever the shoulder and the arm moves, it is more like constantly trying to balance a soccer ball on our foreheads. What then, protects the golf ball from tipping off the “tee” or the soccer ball from falling off our foreheads? — This is achieved via a specialized set of flexible “netting structure” surrounding the shoulder joint. The first layer of protection comes from a flimsy supple sac that encloses the shoulder – the capsule. The dish of the “tee” (glenoid) is further deepened slightly by a raised bumper-like fibrocartilaginous material that circumferentially attaches to the periphery of this tee – the labral ligament. Covering the top of the golf ball, much like a hat, is a special set of tendons. These are the four rotator cuff tendons – one from the front of the shoulder, three from the back of the shoulder. These four tendons, although originate from four different muscles at four different locations, essentially function as one muscle unit, working together in unison. Job of the rotator cuff is to stabilize the shoulder joint when the shoulder moves from one direction to another. The rotator cuff muscle that originates from the front of the shoulder, the subscapularis, is three times stronger than each one of the other three rotator cuff muscles that originate from the back of the shoulder (supraspinatus, infraspinatus, teres minor). That is why it takes three in the back to balance out the one in the front. These four rotator cuff tendons are like legs of an octopus, flexible yet strong. Each leg must dynamically adjust to changes in direction as the shoulder moves, and stiffen up in accordance to which direction the shoulder moves. In order to ensure shoulder stability, all four muscles must contract synergistically in a balanced manner, with just the right amount of tension from each muscle, to keep the humeral head centered and compressed against the glenoid (the golf ball seated and centered on top of the tee) at all times during active shoulder motion. This is termed “glenohumeral joint compression”, or the “centration” effect. Any imbalanced weakness from one of the “legs” of the rotator cuff tendon will lead to asymmetric compression, and will result in subtle wobble of the golf ball off the edge of the tee. This is “microsubluxation” of the shoulder. When repeated hundreds and thousands of times, such as in pitching and throwing, the shoulder will be at risk for peripheral tearing of the labrum, shoulder impingement, bursitis, tendinitis, and tendon tearing.
Functionally, the rotator cuff muscles facilitate 3 aspects of shoulder activity — 1) arm moving to different directions, 2) arm acceleration, and 3) arm deceleration.
When the arm is moving backwards, as in the cocking phase at the start of the throwing sequence, the leverage effect of the entire arm is to push the humeral head forward to slip it off the glenoid anteriorly , off the front of the glenoid. In order to prevent the humeral head from being pushed off the front edge of the glenoid, the front rotator muscle, the subscapularis, must contract hard while being stretched by the arm that is moving backwards (called “eccentric” contraction). This tight contraction by the subscapularis in front of the shoulder compresses the humeral head to maintain centralized position of the humeral head, analogous to forming a tight wall in the front, fighting against the forward moving pressure of the humeral head caused by the leverage effect of the arm moving backwards. Simultaneously, the three posterior rotator cuff muscles must all contract, in a synergistic fashion, maintaining perfect balance so that the humeral head is not moving excessively to either the front or the back of the glenoid.
When the arm is accelerating forward, as in the midst of the throw, the opposite occurs. The forward moving arm diagonally across the body creates a leverage force that pushes the humeral head posteriorly initially, and then is followed by a forward moving shear force due to the entire arm being thrown forward. The surrounding rotator cuff muscles must rapidly adjust to these split second changes of directionality changes. Weak, or imbalanced, rotator cuff muscles will result in pathological wobble of the humeral head with each overhead movement. This microsubluxation causes asymmetric edge loading stress of the humeral head against the rim of the glenoid. The overhead athlete will then eventually suffer from shoulder pain, labral tears, impingement tendinitis, bursitis, tendon fraying and even tendon tearing.
The Challenge Faced By Baseball Players
In addition to cat-like reflexes, arm throwing velocity is a prerequisite for baseball performance. The crown jewel investment of any baseball team is the pitcher. As part of the deal, the pitcher is given the highest demand for throwing, for both the intensity and volume. Second on the list of volume and intensity of throw is the catcher, and lastly, the positional player.
The faster the arm whips, the faster and more impressive the throw. Unlike pitching the baseball, where more than 70% of the power is transferred from the ground up, positional players who execute jump throws in midair do not have the luxury of a ground reactive force to transfer power. The jump throws occur in midair, with both feet off the ground obligating 100% of the power from the shoulder. Fortunately, jump throws are relatively infrequent, and most throws do take advantage of the foot contact ground reactive force transfer. The exception being the catcher. The catcher’s throw may be more of a hybrid with some ground contact force transfer, but throwing power may be at times rely purely from the shoulder depending on body position.
Arm velocity is predicated on a stable shoulder joint, which serves as the stable platform against which the arm can accelerate from, much like the runner pushing off from the starting block at the start of a 100 yard dash. The more stable the platform, the faster the acceleration. Shoulder stability, in turn, is dependent on rotator cuff engagement. Just like race cars, where the engine starts the process, but ultimately the performance rests on a set of good tires. The rotator cuff is the tire to the race car.
Shoulder injury is directly proportional to the number of throws and velocity of the throw. This combination of volume and intensity determine the ultimate failure point for the shoulder. A player who usually throws at 80 mph suddenly line drives 90 mph may be at risk for one event failure because of breakthrough intensity of that particular throw velocity. On the other hand, a pitcher who pitches comfortably at 90 mph average for 80 pitches ramps up to 100 pitches will also suffer injury because of breakthrough volume. As long as the rotator cuff is able to stabilize and engage the shoulder for velocity and total volume, the shoulder will be at less risk of injury. Since all elite baseball players have strong arms able to cover the distance of throw with intensity, the factor that determines failure rests on the volume. This is exactly why those players who are at most risk for shoulder injuries are pitchers. Pitch count is one way of mitigating the volume. Positional players are faced with substantially less volume with less cumulative stress to their shoulders and, therefore, are at less risk for shoulder injuries. Catchers, again being the exception, they have high volume throws, just like the pitcher, but lower intensity except for moments of shear excitement. So, the catchers are second to the pitchers in developing shoulder injuries. Positional players being the least.
Shoulder Throwing Biomechanics
The throwing motion (Figures 1 and 2) is initiated by (1) the wind up phase, with primarily front leg preparation of bringing the leg up to initiate the kinematic chain of events that follow. Then, (2) early cocking, dominated by scapula preparation of squeezing the scapula back to prepare the position of the shoulder glenohumeral joint for ball delivery. Chapman’s over 100 mph pitch has a hip to shoulder separation of beyond 60 degrees with the back shoulder behind midline greater than the average pitcher of being about 50 degrees. (3) Late cocking is when the glenohumeral joint is in maximal external rotation getting ready to launch the projectile. 4) Acceleration phase starts when the arm explodes into internal rotation from that maximally externally rotated position previously set at late cocking. Acceleration phase ends upon ball release and is transitioned rapidly into deceleration phase. All the while, the body propels forward with average stride length of 87% body height with a speed of about 0.9 seconds. Chapman’s 105 mph pitch stride length is 120% his body height in under 0.8 seconds. 5) Deceleration phase is by far the most crucial time for rotator cuff performance. All four rotator cuff muscles must fire simultaneously and synergistically contract to compress the humeral head against the glenoid with a force of about 100 lb in under 50 milliseconds to resist an anteriorly moving shoulder separation force of 50% of the pitcher’s body weight. 100 lb under 50 milliseconds for an arc of motion of the arm of about 4 feet translates into a rotator cuff engagement power of nearly 8,000 ft-lb per second! This is equivalent to the power of a Yamaha 15 horsepower outboard motor for the fishing boat. 6) The final, follow through phase, is completed when the body has restored balanced equilibrium with both feet on the ground getting ready to stop that line drive ball firing back at 100 mph.
Figure 1
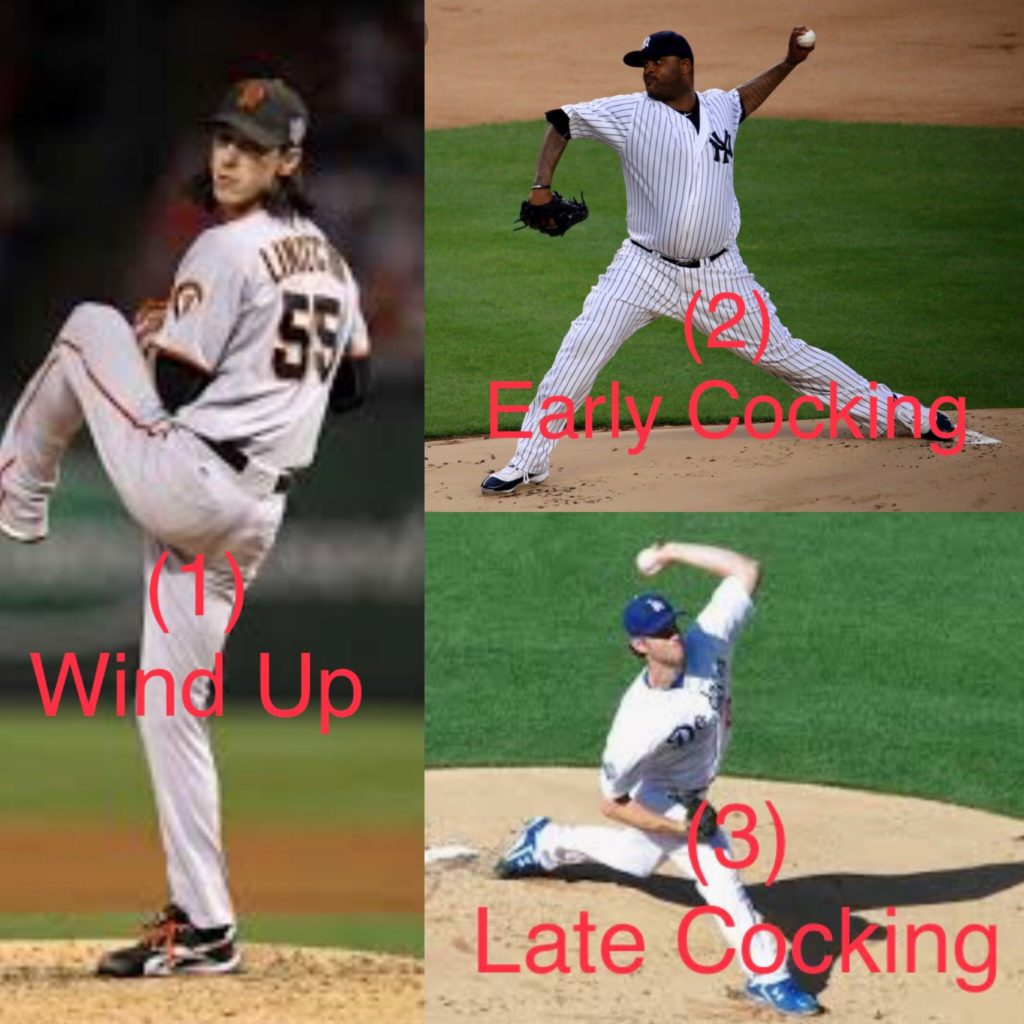
Figure 2

With an arm throwing velocity over 90 mph, these movements are completed in under a tenth of a second. During acceleration phase, elite pitchers can generate shoulder rotational angular velocities of up to 7,600 degrees per second. That is, over 20 revolutions of the arm per second, or 1,200 revolutions per minute. This is the spin cycle speed of a front-loading washing machine, faster than your typical top-loading washing machine!
Absolute shoulder stability is a prerequisite for late cocking phase prior to the initiation of shoulder acceleration. The level of shoulder performance and arm velocity rest upon the ability of the rotator cuff muscles to maintain a stable glenohumeral joint that is centered and compressed prior to acceleration. Acceleration can only be delivered against a stable platform; just like the starting block for footraces or swim races. Shoulder injury prevention relies on a powerful rotator cuff during the deceleration phase that keep the shoulder joint compressed against an over 100 lb shoulder separation force in under a tenth of a second.
A strong and dynamically engaging rotator cuff improves shoulder performance, arm velocity, and prevents shoulder injury.
To achieve this maximal velocity, the shoulder must achieve extreme range of motion in order to deliver motion through the greatest arc of motion. This extreme range of motion comes at a cost of shoulder instability and subluxation.
What makes the rotator cuff exceptionally prone to injury is not just the power required, but the rapid adjustments needed responding to changes in directions of shoulder movement. Within milliseconds, the tendons must adjust to directional changes and stay engaged while the arm whips across sagittal, coronal, and transverse planes of motion. Ineffective and, or, inefficient rotator cuff engagement are direct causes for shoulder instability, shoulder underperformance, shoulder pain, and shoulder injury.
SLAP Tears – A Unique Proposition
An entity unique to throwing athletes is the SLAP tear. SLAP stands for Superior Labrum Anterior and Posterior tear. It is a detachment of the top part of the fibrocartilaginous rim from the shoulder socket (glenoid) where the biceps tendon attaches. Tears can occur from 1) a direct fall onto an outstretched arm, 2) repetitive overhead activity with inadequate shoulder stability, or 3) reflexive biceps muscle eccentric contraction creating tensile stress on the biceps anchor in an unstable shoulder. All overhead athletes are at risk due to the repetitive forceful distracting nature of their sporting events. The greater the intensity and volume of motion, the greater the risk. Among professional baseball players, only about one in three are able to return to their previous level of play after repair of their SLAP tears. However, within subgroups, the positional players faired much better than the pitchers. About 80% of positional players are able to return in contrast to less than one in six for pitchers. This is a testimonial to the intensity and volume pitchers face.
The single most important predictor for shoulder pain and SLAP tear is a weak rotator cuff. Rotator cuff muscles function as eccentric decelerators to maintain “centration” of the shoulder — a shoulder joint that is properly centered by the compression forces created by all four rotator cuff muscles contracting simultaneously. A shoulder during motion, especially at end ranges of motion — such as when the arm is maximally cocked backward at the beginning of the throw, or when maximally stretched forward at the end of the throw, is especially at risk for slippage and rely on this centration effect to keep the shoulder joint properly located.
How To Prevent Baseball Shoulder Injuries
Of the multiple etiologies contributing to shoulder pain and injury, such as scapular dysfunction or neurovascular structures, by far the most important predictor of them all is rotator cuff weakness. Consequently, the cornerstone for all shoulder injury prevention programs is to strengthen the rotator cuff. Traditionally these have involved pulling elastic bands or lifting dumbbells. However, more important than to “strengthen” the four rotator cuff muscles, is to “train” how the four muscles function in unison to effect the desired movement. Therein lies the difference between “strengthening” and “training”. Strengthening gets the muscle strong; training gets the muscle functional for a specific activity. Shoulder injuries among overhead athletes are secondary to poor “motor control”, not “motor weakness”. Elastic bands and weights do “strengthen” the rotator cuff muscles; however they do not “train” for function of the activity across multiple planes of motion, such as throwing a baseball. When the shoulder moves through multiple planes of motion, each rotator cuff tendon must be responsive to changes in shoulder direction, shoulder acceleration, and shoulder deceleration. The function of rotator cuff is to maintain shoulder joint stability throughout all ranges of shoulder motion. This can only be achieved by coordinated synergistic activation of all four rotator cuff muscles, just like a well orchestrated symphony, working together as one functional muscle unit. This “one” functional equivalent muscle unit exerts a constant and well balanced glenohumeral joint compression force through all planes of motions in order to ensure shoulder joint stability and to avoid shoulder injury.
The ShoulderSphere Technique
Rather than pulling rubber bands or lifting dumbbells in a “linearly” directed fashion in one of four “directionally” based movements – the push, pull, lift, or the press; ShoulderSphere (Figure 3) is the only rotator cuff exercise device in the world that strengthens and trains ALL four of the rotator cuff muscles simultaneously in a rotational manner. Linear movements only work on one muscle, one plane, and one direction at a time. These are nonfunctional and may result in imbalanced strengthening.
The use of ShoulderSphere involves active rotation of the ball inside the globe of the ShoulderSphere. When rotating the ball inside the globe in a circular motion, all surrounding muscles must work in a synchronized and balanced fashion in unison in order to to make this circular motion. Any rotator cuff shut down or imbalance will cause the ball inside the globe to drop and bounce rather than to rotate. Additionally, when using the ShoulderSphere, the user’s wrist is locked in the splint by the strap, all the work needed to rotate the ball must all come from the four rotator cuff muscles. The elbow only goes up and down. The wrist, being locked, cannot compensate to rotate the ball. Therefore, all the rotation must come from the rotator cuff…. the rotator cuff rotates. These features make ShoulderSphere the singular rotator cuff exercise device being the most selectively isolated rotator cuff workout of any technique available.
Figure 3

The Electronic Power Tracker
A unique feature of ShoulderSphere is the attached electronic power tracker (the blue box in Figure 1). This electronic tracker gives real-time display of the power of rotator cuff muscles during workouts. Power is equal to arm velocity. Green light equates to low power for endurance workout, red light equates to high power workout for high intensity interval training style exercises (HIIT).
The power tracker is activated by active spinning of the ball inside the ShoulderSphere. The DIRECTION of spin does not matter. Since this is “circular” training, as long as the ball spins, ALL rotator cuff muscles are engaged. The principle of ShoulderSphere workout is to maintain a continuous smooth spin of the ball inside the ShoulderSphere throughout the entire training session. Avoid allowing the ball to bounce, which signifies one or more of the rotator cuff muscles has been shut down, thus the chain of the circle has been broken.
THE POWER TRACKING LIGHT—
Fast spinning makes the power light turn on in red, lower power velocity spin changes it to green. A test, and means of tracking one’s progress with strength improvement, is one’s ability to maintain the tracker lit in red for 30-60 seconds continuously. This is high intensity interval training. Fun gauge regarding one’s own progress. GREEN light can be thought of as endurance training; RED light as power training. Activity translational equivalents can be thought of as that when the power tracker light is maintained in red for 3 second while using the larger ShoulderSphere (A7 model), it is equivalent to the rotator cuff engagement required for an arm velocity of 90 mph throwing a 5 oz baseball 60 feet. When the light is lit in green, it is equivalent to the rotator cuff engagement for an arm velocity of 60 mph throwing a 5 oz baseball 60 feet.
Strengthening vs Training
ShoulderSphere can be used either as a pure rotator cuff strengthening device (in “static mode”), or as a training device (in “dynamic mode”). “Static mode” technique to strengthen the rotator cuff is performed by active rotation of the ball inside the globe without concurrent arm motion. “Dynamic mode” training technique is performed by moving the arm through various planes of motion while at the same time rotating the ball inside the globe (which actually also strengthens the rotator cuff muscles at the same time). Dynamic mode specifically trains the responsiveness of the rotator cuff muscles to adjust to the changing directions of multiplanar shoulder movements. All four rotator cuff muscles are trained to function as one muscle unit, not separately as four, to maintain glenohumeral joint compression at all times. This trains motor control and constant rotator cuff engagement for those ranges of motion. The following video depict “Static mode” training and “Dynamic mode” training.
https://www.youtube.com/watch?v=5cDhUslv4xA
https://www.youtube.com/watch?v=H6IJV9ebJDQ
Of particular importance for any throwing activity is controlled rotator cuff engagement at end ranges of motion — these are at the start of cocking phase and the terminal follow-throw phase when subluxations occur. Failure of shoulder with subluxation is due to failure of eccentric rotator cuff contraction in the front of the shoulder during cocking, or the back of the shoulder during follow-throw. Consequently, paramount for shoulder injury prevention is eccentric training, ie train deceleration power of the rotator cuff muscles to stay engaged for these positions.
Training the Rotator Cuff For Athletic Shoulder Movements
Shoulder injuries among overhead athletes are due to poor “motor control”, not due to lack of “motor strength”. Strength is how strong you are in one plane; control is how you well can move your arm through multiple planes. To be truly functional is the ability to adjust and maintain stability of the shoulder in a multidirectional manner when the arm is rapidly moving through changes in planes of motion.
The ShoulderSphere technique specifically builds rotator cuff power with training for control. This is performed by mimicking event-specific movements of the arm that mirror the athletic motor patterns involved, such as in throwing or batting. This “dynamic” motor control workout calls for active rotation of the ball inside the ShoulderSphere globe while the arm mimicks the athletic pattern intended. The closer the mimicked motion that mirrors the activity intended, the more powerful will be the motor control training for rotator cuff responsiveness to stabilize the shoulder for that intend activity. These video links demonstrate motor control training of rotator cuff responsiveness for baseball specific movements.
https://www.youtube.com/watch?v=wrvQxxU2Es4
https://www.youtube.com/watch?v=6eVTYLEYf_s
ShoulderSphere is the most efficient and effective rotator cuff training device you will ever need. After all, it is not how hard you train, but how smart you train. Knowing the why how you train, for what you train, will make all the difference in the world separating a champion from everyone else. ShoulderSphere is indeed the toughest rotator cuff training device that all athletes love.
Here is the link for a 10-week progressive rotator cuff strengthening program for baseball players.
To learn more about ShoulderSphere and how you can integrate various strengthening and training techniques to suit your needs, please visit www.ShoulderSphere.com and follow us on Instagram or Twitter @ShoulderSphere. Dr. Chang is also available to assist with any questions or special needs at Win@ShoulderSphere.com.